The Existence of Pain Receptors in the Skin
Pain is perhaps the most misunderstood of our senses. While often viewed as an antagonist to human comfort, it is, in reality, a sophisticated biological achievement. The ability to perceive noxious stimuli—a process known as nociception—is a fundamental survival mechanism that allows organisms to detect and avoid harm.1 At the center of this protective system is a specialized network of sensory neurons embedded within the skin: the nociceptors.
1. Defining the Nociceptor: The Body’s Alarm System
The term “nociceptor” was coined by the Nobel Prize-winning physiologist Sir Charles Sherrington to distinguish these specialized neurons from those that respond to harmless stimuli, such as a light breeze or a gentle caress.2
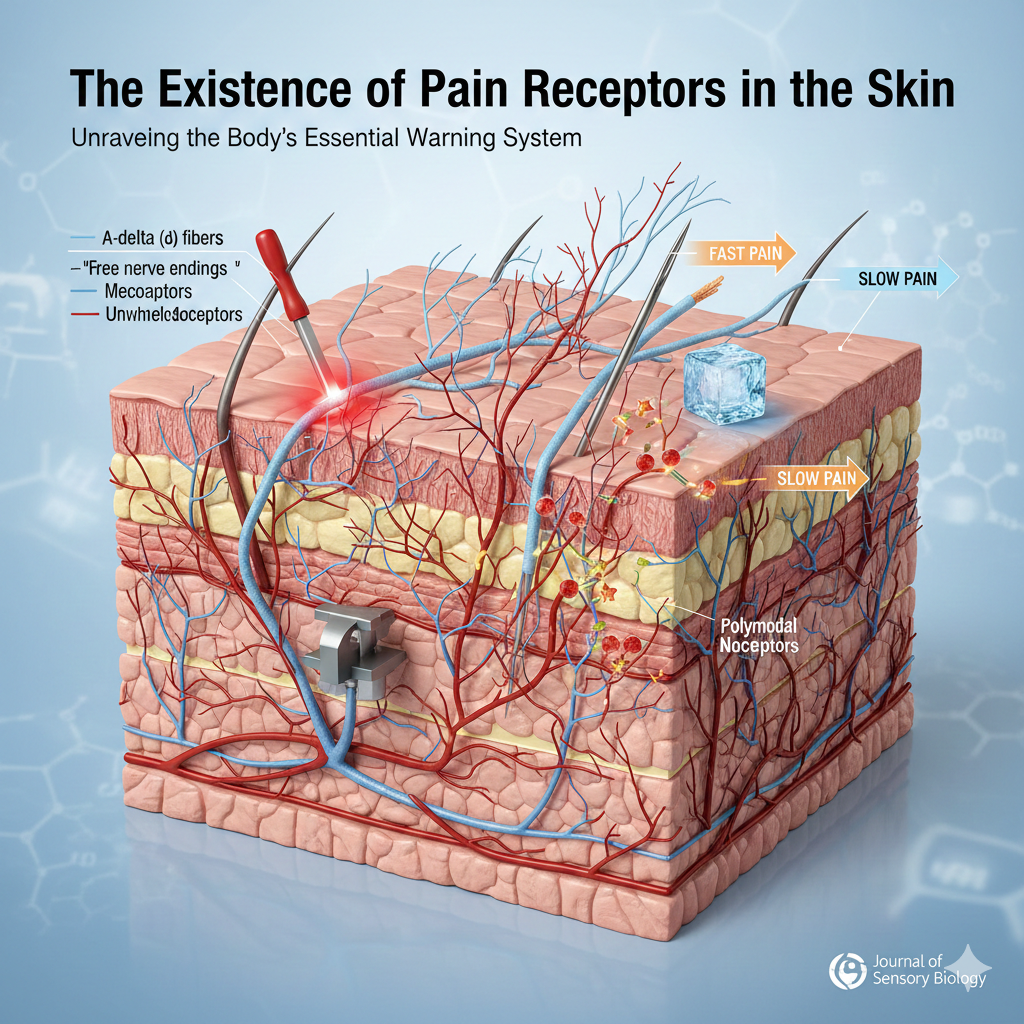
Unlike other sensory receptors (like those for sight or hearing), nociceptors are “free nerve endings.”3 They do not possess the complex, encapsulated structures seen in other skin receptors like Meissner’s corpuscles (which detect touch) or Pacinian corpuscles (which detect vibration). Instead, these bare axons branch out into the layers of the skin, acting as high-threshold sensors that only “fire” when a stimulus reaches a level that could potentially cause tissue damage.4
2. The Anatomy and Distribution in the Skin
The skin is the largest organ of the human body and serves as our primary interface with the external world.5 To protect this interface, nociceptors are strategically distributed throughout its layers:
The Epidermis
The outermost layer of the skin contains a high density of free nerve endings.6 Because the epidermis is the first point of contact for external threats (like a hot stove or a sharp needle), these receptors provide the quickest possible warning to the central nervous system.
The Dermis
Beneath the epidermis, the dermis contains a rich supply of blood vessels, hair follicles, and a more complex network of nociceptors. Pain originating here is often more intense and can be triggered by deeper mechanical pressure or chemical changes resulting from inflammation.
3. Classification of Pain Receptors
Not all pain is created equal, and our skin uses different types of nociceptors to categorize the nature of a threat. These are broadly classified based on the stimuli they respond to and the speed at which they conduct signals.7
A. Thermal Nociceptors
These are activated by extreme temperatures.8 Most humans begin to perceive pain when the skin surface temperature exceeds $45°C$ ($113°F$) or falls below $5°C$ ($41°F$). These receptors utilize specialized ion channels, such as TRPV1 (heat) and TRPM8 (cold), to convert thermal energy into electrical impulses.
B. Mechanical Nociceptors
These respond to intense physical deformation of the skin. This includes stretching, cutting, or pinching. They are essential for identifying the location and severity of physical trauma.9
C. Chemical Nociceptors
These receptors respond to a wide variety of chemical stimulants.10 This includes exogenous substances (like the “heat” in chili peppers, caused by capsaicin) and endogenous substances released by the body during injury, such as bradykinin, histamine, and prostaglandins.
D. Polymodal Nociceptors
The most common type of pain receptor in the skin is the polymodal nociceptor. As the name suggests, these are versatile sensors capable of responding to high-intensity mechanical, thermal, and chemical stimuli.11
4. The Physiology of a “Ouch”: Transduction and Transmission
The journey from a physical injury to the conscious perception of pain involves a complex sequence of biological events.
Step 1: Transduction
When you step on a LEGO brick, the mechanical pressure causes the membranes of the nociceptors in your foot to stretch. This physical change opens ion channels, allowing positively charged ions to flow into the neuron. This shifts the electrical charge of the cell, creating an action potential.
Step 2: Transmission via A-delta and C-Fibers
The signal travels from the skin to the spinal cord via two distinct types of “cables”:
- A-delta (12$\delta$) Fibers: These are thinly myelinated (insulated) axons.13 They conduct signals rapidly ($5$ to $30$ meters per second). They are responsible for the “first pain”—the sharp, localized sting that happens immediately upon injury.14
- C-Fibers: These are unmyelinated and much thinner.15 They conduct signals slowly (less than $2$ meters per second). They produce the “second pain”—the dull, aching, or throbbing sensation that lingers long after the initial impact.
5. The “Inflammatory Soup” and Sensitization
When tissue is damaged, the area around the pain receptors becomes a site of intense chemical activity. Cells at the site of injury release a cocktail of chemicals often referred to by neuroscientists as the “inflammatory soup.”
This soup includes:
- Serotonin and Histamine: Released from mast cells and platelets.16
- Prostaglandins: Which lower the threshold of the nociceptors, making them more sensitive.17 This is why a sunburned shoulder hurts even when touched lightly—a phenomenon known as allodynia.
Modern pain medications, such as Ibuprofen or Aspirin, work by inhibiting the enzymes (COX-1 and COX-2) that produce prostaglandins, effectively “quieting” the receptors at the source.
6. Clinical Importance: When Pain Receptors Fail
The absolute necessity of pain receptors is best illustrated by their absence. Congenital Insensitivity to Pain (CIP) is a rare genetic disorder where individuals are born with non-functional nociceptors or a failure in the pain-signaling pathway.18
While it may sound like an advantage to never feel pain, the reality is devastating. Children with CIP often bite off pieces of their tongues, suffer from undetected bone fractures, and may experience severe burns because their bodies do not tell them to pull away from heat.19 Without the “existence of pain receptors,” the body loses its most critical guardian.
7. Conclusion
The existence of pain receptors in the skin is not merely a biological fact; it is a sophisticated defense system. Through the coordinated efforts of A-delta and C-fibers, and the sensitivity of various nociceptor types, our skin acts as a high-tech security perimeter. Understanding these receptors is the key to developing better treatments for chronic pain and appreciating the complex biological dialogue that keeps us safe every day.
Quran already mentioned about this. Read Chapter An Nisa: 56 : “Indeed, those who disbelieve in Our verses – We will drive them into a Fire. Every time their skins are roasted through, We will replace them with other skins so they may taste the punishment. Indeed, Allah is ever Exalted in Might and Wise.”
Read also The Miracle of the Fingertip and Embryonic Development in Stages
Authoritative References & Further Reading
For those seeking to explore the rigorous science behind nociception, the following resources provide peer-reviewed data and comprehensive overviews:
- NCBI Bookshelf – Neuroscience (2nd Edition):Nociceptors. This text provides the foundational biological details on how these receptors function.
- The International Association for the Study of Pain (IASP): The global authority on pain terminology and classification.
- Nature Reviews Neuroscience:Nociceptors: The Sensors of the Pain Pathway. This article discusses the molecular transducers that allow nociceptors to detect heat, cold, and chemicals.
- The Journal of Clinical Investigation:The Molecular Biology of Pain. A deep dive into the ion channels (like TRPV1) that facilitate pain transduction.
- The Mayo Clinic:How Pain Works. A patient-focused explanation of the nervous system’s role in pain perception.

